Gallbladder Ultrasound
Introduction
Gallbladder ultrasound is the primary imaging modality for evaluating biliary pathology due to its:
- High sensitivity (91-97%) for gallstones
- Real-time imaging capabilities
- Absence of ionizing radiation
- Bedside availability
Anatomy of the gallbladder
Location: Gallbladder fossa (inferior surface of liver segments IV/V).
Parts:
- Fundus: Rounded blind end projecting beyond liver margin
- Body: Main contact area with liver
- Neck: Tapers into cystic duct (spiral valves of Heister)
- Dimensions: 7-10 cm long, 2.5-4 cm wide
Clinical indications
1. Basic indications for Gallbladder Ultrasound
- Right upper quadrant (RUQ) pain
- Suspected cholelithiasis
- Jaundice evaluation
- Abnormal liver function tests
- Fever of unknown origin (rule out cholecystitis)
2. Specific Clinical Scenarios
- Acute cholecystitis: RUQ pain + fever + Murphy's sign
- Choledocholithiasis: Jaundice + elevated ALP/GGT
- Gallbladder polyps: Incidental finding, often asymptomatic
Scanning Technique and Preparation
1. Patient Preparation
Ingestion of food, particularly fatty food, stimulates the gallbladder to contract. The contracted gallbladder appears thick walled and may obscure luminal or wall abnormalities. Therefore the examination of the gallbladder should be performed after a minimum of 4 hours of fasting.
Fasting Protocol
- <4 hours: Leads to contracted gallbladder, may lead to false-negative for stones/sludge
- 6-8 hours (ideal): Maximal distension, optimal visualization
- >12 hours: May lead to sludge formation, which can mimic pathology
2. Equipment Settings
- Transducer: Curvilinear (3-5 MHz) for adults, higher frequency for pediatrics
- Depth: Adjust to include entire gallbladder and porta hepatis
- Focal zones: Set at level of gallbladder fossa
- Harmonic imaging: Improves contrast resolution (recommended)
3. Systematic Scanning Approach
- Subcostal view: Identify gallbladder in longitudinal and transverse planes
- Intercostal view: Alternative approach for high-lying gallbladders
- CBD evaluation: Trace from gallbladder neck to pancreatic head
- Dynamic maneuvers: Patient rotation, deep inspiration
Normal Sonographic Findings
1. Gallbladder
- Pear-shaped anechoic structure
- thickness <3 mm
- No internal echoes (except dependent sludge)
- Normal length 7-10 cm, width <4 cm
2. Bile Ducts
- Walls appear as thin echogenic lines
- Lumen is anechoic
- No intraductal masses or calculi
- No periductal edema or vascularity
Landmark: Portal Triad
The "Mickey Mouse" sign represents the portal triad in cross-section:
- Head: Hepatic artery (smallest)
- Left ear: Common bile duct
- Right ear: Portal vein (largest)

Normal gallbladder
Thin-walled (typically less than 3mm thick), anechoic (appears dark or black) structure that is pear-shaped and measures around 7-10cm in length and 3-4cm in width
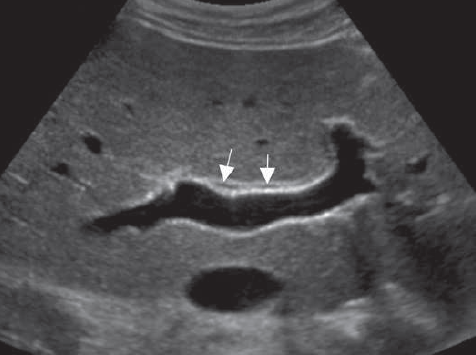
Normal Bile Ducts
Right and left hepatic ducts (short arrows) are normally seen lying anterior to the portal veins. Appear anechoic without any signs of dilation or obstruction
Pathological Findings
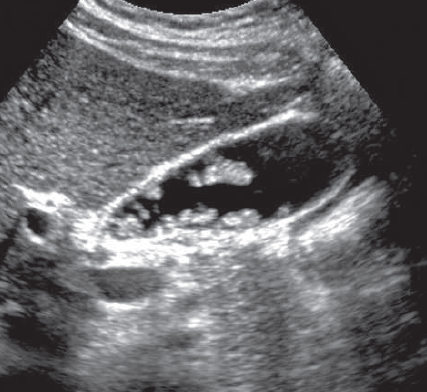
1. Cholelithiasis (Gallstones)
- Findings: Mobile hyperechoic focus with posterior shadowing
- WES triad: Wall-echo-shadow in contracted gallbladder
- Complications: Cholecystitis, empyema, porcelain gallbladder
2. Biliary Sludge: Is a mixture of particulate matter and bile that occurs when solutes in bile precipitate. It appear as amorphous, low-level echoes within the gallbladder in a dependent position, with no acoustic shadowing.
3. Acute Cholecystitis
- Gangrenous Cholecystitis. Irregular gallbladder wall with small collections within the wall that may represent abscesses or hemorrhage. There is also nonlayering bands of echogenic tissue within the lumen representing sloughed membranes and blood
- Perforated Gallbladder. The focus of perforation, seen as a small defect in the wall of the gallbladder or rent in the wall of the gallbladder, is often visible. Clues to perforation are the delation of the gallbladder, with loss of its normal gourdlike shape, and a focal pericholecystic fluid collection.
- Emphysematous Cholecystitis. The sonographic appearence is as a result of gas produced by gas-forming bacteria, presumably after an ischemic event affecting the gallbladder. Can appear as echogenic lines, with posterior dirty shadowing, reverberation, or ring-down artifact
- Acalculous Cholecystitis.
4. Torsion (Volvulus) of Gallbladder. The hallmarks on imaging are a massively distended and inflammed gallbladder lying in an unusual horizontal position, with its long axis oriented in a let-to-right direction. A twist of the cystic artery and cystic duct may be visible. If the torsion is greater than 180 degrees, gangrene of the gallbladder ensues; otherwise, obstruction of the cystic duct and acute cholecystitis occur. In either case, treatment is usually surgical.
5. Chronic Cholecystitis. Is associated with the mere presence of gallstones; therefore patients are usually asymptomatic and have mild disease.
6. Porcelain Gallbladder. Calcification of the gallbladder wall is termed porcelain gallbladder. Its cause is unknown, but it occurs in association with gallstone disease and may represent a form of chronic cholecystitis. The degree and pattern of calcification determine the sonographic appearance; When the entire gallbladder wall is thickly calciied, a hyperechoic semilunar line with dense posterior acoustic shadowing is noted. Mild calciication appears as an echogenic line with variable degrees of posterior acoustic shadowing. he luminal contents may be visible. Interrupted clumps of calcium appear as echogenic foci with posterior shadowing
7. Adenomyomatosis (Adenomatous Hyperplasia). Adenomyomatosis may be focal or difuse. The most common appearance on sonography is tiny, echogenic foci in the gallbladder wall that create comet-tail artifacts, presumably caused by either the cystic space itself or the internal debris
8. Polypoid Masses of Gallbladder
- Cholesterol Polyps. Appear as multiple ovoid, nonshadowing lesions attached to the gallbladder wall
- Adenomas, Adenomyomas, and Inflammatory Polyps. These are usually pedunculated, and larger lesions may contain foci of malignant transformation.98 Adenomas tend to be homogeneously hyperechoic but become more heterogeneous as they increase in size
9. Malignancies

Cholelithiasis
- Mobile hyperechoic focus with posterior shadowing.

Cholelithiasis (WES triad)
- Wall echo shadow in a contracted gallbladder
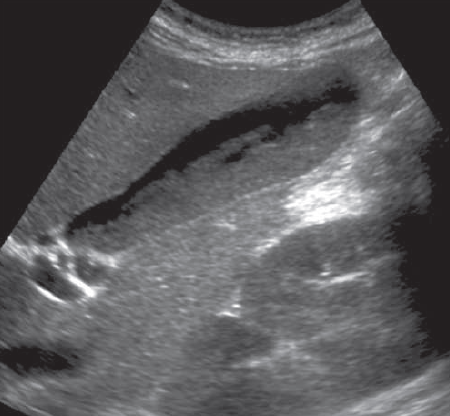
Gallbladder sludge
- Tumefactive sludge
- Sagittal sonogram shows gallbladder filled with tumorlike sludge.

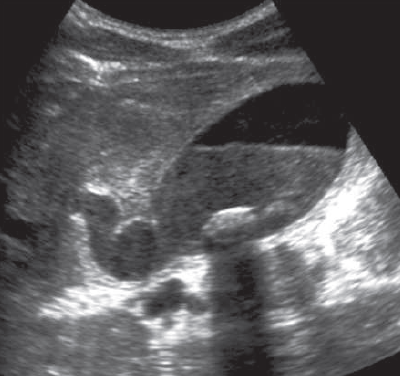
Gallbladder sludge
- Hepatisation of gallbladder
- Internal echoes within the gallbladder mimic the normal liver parenchyma
- Normal gallbladder wall
Acute cholecystitis
- Tense distended gallbladder
- Wall thickening
- Fluid-debris level
- Nonobstructive stone with posterior acoustic shadowing.
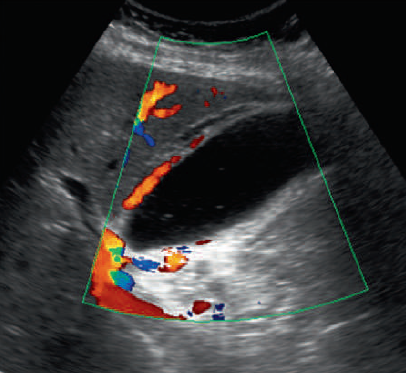
Acute cholecystitis
- Prominent cystic artery and hyperemia in the wall of the gallbladder as well as the adjacent liver on color doppler application.

Porcelain gallbladder
- Calcified gallbladder with posterior acaustic shadowing
- This appearance could be mistaken for a stone within the gallbladder lumen. There is, however, no gallbladder wall supericial to the echogenic focus.
Gallbladder polyp
- Multiple non-mobile small sized tumors in the gallbladder lumen originating from the gallbladder wall.
References
- American College of Radiology (ACR). (2023). ACR Appropriateness Criteria® Right Upper Quadrant Pain. Journal of the American College of Radiology, 20(1S), S12-S24.
- Middleton, W. D., et al. (2022). Ultrasound: The Requisites (4th ed.). Elsevier.
- Rumack, C. M., & Levine, D. (2021). Diagnostic Ultrasound (6th ed.). Elsevier.
- National Institute for Health and Care Excellence (NICE). (2022). Gallstone disease: diagnosis and management. NICE Clinical Guideline 188.
- European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB). (2021). Guidelines on Interventional Ultrasound. Ultraschall in der Medizin, 42(1), 12-45.