Ultrasound of Acute and Chronic Appendicitis
Introduction
Appendicitis is one of the most common causes of acute abdominal pain requiring surgical intervention. Ultrasound serves as an excellent first-line imaging modality, particularly in children, young adults, and pregnant women where radiation exposure is a concern. This article reviews the ultrasound features of both acute and chronic appendicitis.
Clinical Presentation
Patients with appendicitis typically present with:
- Acute appendicitis:
- Periumbilical pain migrating to right lower quadrant (RLQ)
- Anorexia
- Nausea/vomiting
- Low-grade fever
- Rebound tenderness and guarding
- Chronic appendicitis:
- Recurrent or persistent RLQ pain
- Milder symptoms lasting weeks to months
- Often without fever or leukocytosis
Ultrasound findings
Acute Appendicitis
- Non-compressible tubular structure >6 mm in outer diameter (measured from outer wall to outer wall)
- Target sign - Concentric wall layers with hypoechoic muscularis propria
- Wall thickening (>2-3 mm) with hyperemia on color Doppler
- Periappendiceal fat inflammation (hyperechoic fat)
- Appendicolith (hyperechoic focus with posterior shadowing)
- Free fluid around the appendix
- Abscess formation in complicated cases
Chronic Appendicitis
- Fibrotic, thickened appendix wall with loss of layered appearance
- Periappendiceal fat stranding but less pronounced than acute cases
- Lymphoid hyperplasia may be present
- Minimal vascularity on Doppler compared to acute inflammation
- Possible strictures or dilatation of appendiceal lumen

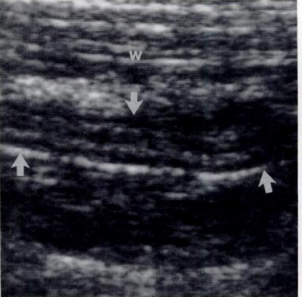
1. Acute Appendicitis
- Non-compressible dilated appendix (8.7mm)
- Wall thickening and hyperechoic periappendiceal fat

2. Appendicolith
- Hyperechoic focus with posterior acoustic shadowing
- Often associated with obstruction leading to appendicitis
3. Chronic Appendicitis
- Thickened fibrotic wall without layered appearance
- Minimal surrounding inflammation

4. Appendiceal Abscess
- Complex fluid collection adjacent to appendix
- Thick irregular walls with debris
Graded Compression Technique
The optimal technique for appendiceal ultrasound involves:
- Use high-frequency linear transducer (5-12 MHz)
- Systematic compression starting from ascending colon
- Identify terminal ileum and psoas muscle as landmarks
- Apply gradual pressure to displace bowel gas and assess compressibility
- Evaluate for secondary signs (fat inflammation, free fluid)
- Use color Doppler to assess vascularity
Diagnostic Criteria Comparison
| Feature | Acute Appendicitis | Chronic Appendicitis |
|---|---|---|
| Diameter | >6 mm | Variable (often 5-7 mm) |
| Wall thickness | >2-3 mm | >2 mm but less edema |
| Wall layers | Preserved (target sign) | Often lost |
| Vascularity | Markedly increased | Mild to moderate |
| Surrounding fat | Markedly hyperechoic | Mild stranding |
| Compressibility | Non-compressible | Partially compressible |
Differential Diagnosis
Several conditions can mimic appendicitis on ultrasound:
- Mesenteric adenitis - Enlarged lymph nodes without appendix changes
- Omental infarction - Hyperechoic non-compressible fat mass
- Diverticulitis - Thickened bowel wall with inflamed diverticulum
- Gynecological pathology (ovarian cyst, PID, ectopic pregnancy)
- Crohn's disease - Terminal ileum involvement with skip lesions
- Typhlitis - Cecal wall thickening in immunocompromised patients
Conclusion
Ultrasound remains a valuable first-line imaging modality for evaluating suspected appendicitis, particularly in pediatric populations and pregnant women. Recognition of key sonographic features allows accurate diagnosis of both acute and chronic forms. While acute appendicitis typically shows marked inflammation, vascularity, and surrounding fat changes, chronic appendicitis demonstrates more fibrotic changes with less pronounced inflammatory markers. Correlation with clinical findings remains essential for accurate diagnosis.
References
- Puylaert JB. Acute appendicitis: US evaluation using graded compression. Radiology. 1986;158(2):355-360.
- Kessler N, et al. Appendicitis: evaluation of sensitivity, specificity, and predictive values of US, Doppler US, and laboratory findings. Radiology. 2004;230(2):472-478.
- Trout AT, et al. Imaging of acute appendicitis in children: AJR Expert Panel Narrative Review. AJR Am J Roentgenol. 2022;219(2):204-214.
- Mostbeck G, et al. How to diagnose acute appendicitis: ultrasound first. Insights Imaging. 2016;7(2):255-263.