Peribiliary cysts
Introduction
Peribiliary cysts are rare, benign cystic lesions that occur in the hepatic hilum and along the larger intrahepatic bile ducts. These cysts develop from the peribiliary glands and are typically discovered incidentally during imaging studies for unrelated conditions.
While often asymptomatic, peribiliary cysts can sometimes lead to biliary obstruction or be mistaken for more serious conditions, making their recognition on ultrasound important for proper patient management.
Ultrasound Features
Key Ultrasound Characteristics
- Multiple small anechoic cysts (typically 0.2-2.5 cm in diameter)
- Location along the portal triads (hepatic hilum and large intrahepatic bile ducts)
- No communication with the biliary tree (unlike Caroli disease)
- Thin, smooth walls without internal septations or solid components
- Posterior acoustic enhancement
- No internal vascularity on Doppler examination
Typical Ultrasound Appearance
On ultrasound, peribiliary cysts appear as multiple small, round or oval anechoic structures clustered around the portal triads. They demonstrate through transmission (posterior acoustic enhancement) and lack internal echoes or septations. The cysts are typically arranged linearly along the course of the bile ducts.
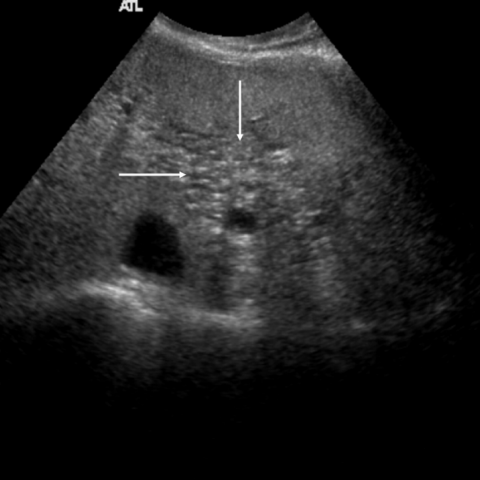
Peribiliary cysts
- Ultrasound image showing multiple small anechoic cysts along portal triads
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Caroli disease | Communicates with biliary tree, may show "central dot" sign |
| Biliary hamartomas | More diffuse distribution, smaller size (usually <1 cm) |
| Simple hepatic cysts | Random distribution, not associated with portal triads |
| Periportal lymphadenopathy | Solid appearance, may show vascularity on Doppler |
Associated Conditions
Peribiliary cysts are more commonly found in patients with:
- Liver cirrhosis (particularly in advanced stages)
- Portal hypertension
- Polycystic liver disease
- Congenital hepatic fibrosis
Management
Management Approach
- Asymptomatic cysts: No treatment needed; periodic monitoring may be considered
- Symptomatic cysts: Consider drainage or surgical intervention if causing obstruction
- Uncertain diagnosis: Follow-up imaging or additional modalities (CT/MRCP) may be warranted
- Associated conditions: Manage underlying liver disease appropriately
Follow-up Recommendations
For incidentally discovered peribiliary cysts:
- If typical appearance and asymptomatic: No routine follow-up needed
- If atypical features or symptoms develop: Consider follow-up ultrasound in 6-12 months or advanced imaging
- For patients with underlying liver disease: Follow-up as indicated for primary condition
Interventional Options
For symptomatic cases causing biliary obstruction:
- Percutaneous cyst drainage (temporary measure)
- Endoscopic cyst unroofing or marsupialization
- Surgical resection (rarely needed, only for refractory cases)
References
- Nakanuma Y, Kurumaya H, Ohta G. Multiple cysts in the hepatic hilum and their pathogenesis. A suggestion of periductal gland origin. Virchows Arch A Pathol Anat Histopathol. 1984;404(4):341-350.
- Itai Y, Ebihara R, Tohno E, et al. Hepatic peribiliary cysts: multiple tiny cysts within the larger portal tract, hepatic hilum, or both. Radiology. 1994;191(1):107-110.
- Terada T, Nakanuma Y. Pathological observations of intrahepatic peribiliary glands in 1,000 consecutive autopsy livers. III. Survey of necroinflammation and cystic dilatation. Hepatology. 1990;12(5):1229-1233.
- Wachsberg RH. Peribiliary cysts: a benign cause of bile duct dilatation that may mimic obstruction. AJR Am J Roentgenol. 1997;168(2):501-502.
- Baron RL, Campbell WL, Dodd GD 3rd. Peribiliary cysts associated with severe liver disease: imaging-pathologic correlation. AJR Am J Roentgenol. 1994;162(3):631-636.