Appendix Ultrasound
Introduction
Appendix ultrasound is the first-line imaging modality for suspected appendicitis, especially in children and young adults, due to its:
- High sensitivity (75-90%) and specificity (90-95%) in experienced hands
- Real-time imaging capabilities with graded compression
- Absence of ionizing radiation
- Bedside availability
Limitations: Operator-dependent technique, may be limited by patient body habitus and bowel gas.
Appendiceal Anatomy
Location: Arises from posteromedial cecum, typically in right lower quadrant (RLQ).
Normal Characteristics:
- Blind-ending tubular structure
- Diameter <6 mm (outer wall to outer wall)
- Wall thickness <3 mm
- Compressible with no surrounding inflammation
- No internal vascularity on Doppler
Variants: Retrocecal (most common variant), pelvic, subhepatic positions
Clinical Indications
1. Common Indications
- Right lower quadrant pain
- Suspected acute appendicitis
- Evaluation of appendiceal abscess
- Pediatric abdominal pain
- Pregnant patients with RLQ pain
2. Specific Clinical Scenarios
- Classic appendicitis: Periumbilical pain migrating to RLQ + rebound tenderness
- Atypical presentations: Pelvic pain, flank pain, or diffuse abdominal pain
- Pediatric cases: Non-specific symptoms (anorexia, vomiting, low-grade fever)
Scanning Technique
1. Patient Preparation
- No fasting required is required
- Patient positioning: Supine, with slight left lateral decubitus tilt if needed
- Communication: Explain graded compression to patient
2. Equipment Settings
- Transducer: High-frequency linear (7-15 MHz) for optimal resolution
- Depth: Adjust to include entire appendix and surrounding structures
- Harmonic imaging: Improves tissue contrast
- Doppler settings: Low PRF (500-1000 Hz) for slow flow detection
3. Systematic Scanning Approach
- Begin at point of maximal tenderness: Usually McBurney's point
- Graded compression technique: Gradually increase pressure to displace bowel gas
- Identify landmarks: Psoas muscle, iliac vessels, cecum
- Trace terminal ileum: To locate appendiceal origin
- Assess entire length: From base to tip
Normal Sonographic Findings
1. Normal Appendix
- Blind-ending tubular structure arising from cecum
- Diameter <6 mm (outer wall to outer wall)
- Wall thickness <3 mm
- Compressible with transducer pressure
- No periappendiceal fat inflammation
2. Surrounding Structures
- Normal echogenic periappendiceal fat
- No free fluid in RLQ
- Normal bowel peristalsis adjacent to appendix
- No lymphadenopathy
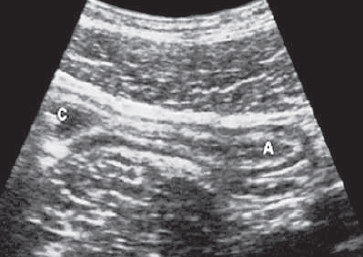
Normal Appendix (Longitudinal)
Blind-ending tubular structure (A) with thin walls (<3mm) and diameter <6mm, originating from the caecum (C).
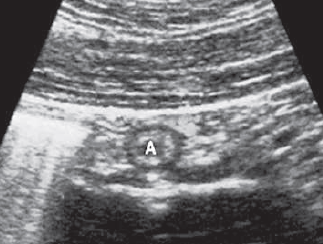
Normal Appendix (Transverse)
Target appearance with concentric wall layers, fully compressible appendix (A).
Pathological Findings
1. Acute Appendicitis
- Primary signs:
- Non-compressible, blind-ending tube >6mm diameter
- Wall thickening (>3mm)
- Hyperemia on Doppler
- Secondary signs:
- Periappendiceal fat inflammation (hyperechoic fat)
- Free fluid in RLQ
- Appendicolith (hyperechoic focus with shadowing)
2. Perforated Appendicitis
- Loss of continuity of appendiceal wall
- Periappendiceal abscess (complex fluid collection)
- Increased surrounding inflammatory changes
- Possible localized pneumoperitoneum
3. Appendiceal Abscess
- Complex fluid collection adjacent to cecum
- Thick, irregular walls with increased vascularity
- Possible gas bubbles within collection
- May contain appendicolith
4. Mucocele of Appendix
- Dilated, fluid-filled appendix without inflammation
- Diameter typically >15mm
- May contain echogenic mucin
- Wall calcifications in some cases
5. Appendiceal Neoplasms
- Carcinoid tumor: Hypoechoic nodule at tip of appendix
- Adenocarcinoma: Irregular wall thickening with loss of layers
- Metastases: Rare, usually from GI or ovarian primaries

Acute Appendicitis (Longitudinal)
- Non-compressible, dilated appendix (>6mm)
- Wall thickening (>3mm)
- Surrounding hyperechoic fat
Acute Appendicitis (Transverse)
- Target sign with thickened walls
- Hyperemic wall on Doppler
- Appendicolith with shadowing

Perforated Appendicitis
- Wall defect
- Periappendiceal abscess
- Marked surrounding inflammation

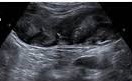
Appendiceal Abscess
- Complex fluid collection (A)
- Thick, irregular walls
- Adjacent inflamed fat
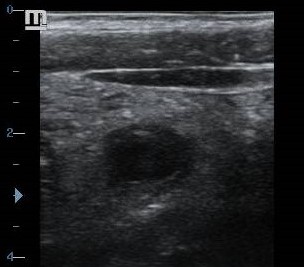
Appendiceal Mucocele
- Markedly dilated appendix
- Thin walls without inflammation
- Echogenic mucin content

Appendiceal Carcinoid
- Hypoechoic nodule at tip (arrows)
- Preserved wall layers of the appendix (A)
- No significant inflammation
References
- American College of Radiology (ACR). (2023). ACR Appropriateness Criteria® Right Lower Quadrant Pain. Journal of the American College of Radiology, 20(1S), S78-S92.
- Puylaert, J. B. (2022). Ultrasonography of the Acute Abdomen (2nd ed.). Springer.
- Rumack, C. M., & Levine, D. (2021). Diagnostic Ultrasound (6th ed.). Elsevier.
- World Society of Emergency Surgery (WSES). (2023). Guidelines for diagnosis and treatment of acute appendicitis. World Journal of Emergency Surgery, 18(1), 1-25.
- European Society of Pediatric Radiology (ESPR). (2022). Imaging guidelines for pediatric appendicitis. Pediatric Radiology, 52(3), 425-438.